Infant and Adult Frenectomy
What is a Frenectomy?
 A frenectomy is a procedure that consists of releasing the frenum under the tongue or upper lip or cheek to allow for better range of motion. Children may be born with a combination of conditions called a tongue-tie (ankyloglossia) and/or a lip/buccal-tie causing restrictions in movement that can cause difficulty with breastfeeding, and in some instances, other health problems like dental decay or spacing, speech and airway difficulties, and digestive issues. These issues can generally be corrected by a simple procedure done with our soft tissue laser.
A frenectomy is a procedure that consists of releasing the frenum under the tongue or upper lip or cheek to allow for better range of motion. Children may be born with a combination of conditions called a tongue-tie (ankyloglossia) and/or a lip/buccal-tie causing restrictions in movement that can cause difficulty with breastfeeding, and in some instances, other health problems like dental decay or spacing, speech and airway difficulties, and digestive issues. These issues can generally be corrected by a simple procedure done with our soft tissue laser.
Smooth breastfeeding is a time to bond between mother and infant and so relaxing for both. On the other hand, difficult breastfeeding can be a time of pain, frustration, and anxiety.
There is hope for these rocky starts to breastfeeding. A mother may not realize the issues may be on the baby’s side with a tongue tie.
And it can be fixed.
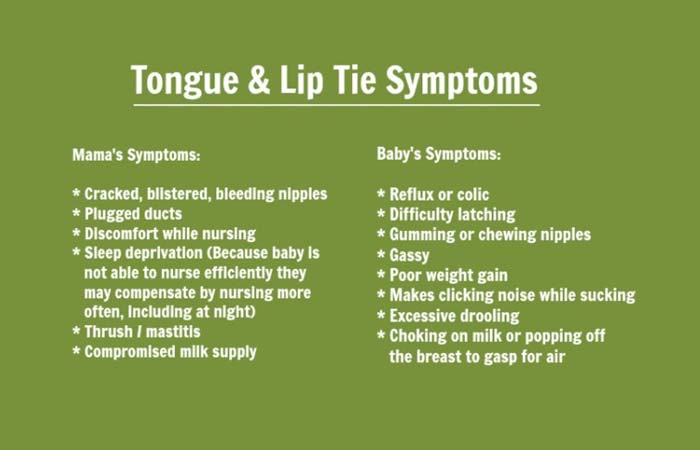
Successful breast-feeding depends on multiple factors. One issue that can adversely affect the newborn’s ability to obtain a correct latch is the presence of a tongue or a lip tie. The flap of tissue under the upper lip and under the tongue is called a frenum. The attachment under the upper lip is the maxillary labial frenum and the one under the tongue is the lingual frenum. An overly attached frenum can cause several baby and mother breastfeeding symptoms.
First infant visit for Tie examination
Dr Mirkal will closely work with your IBCLC[Lactation consultant] to make sure a team of providers have assessed before a thorough diagnosis is made. If you do not have one we can make recommendations.
After a thorough evaluation of your baby’s mouth, you will be presented with objective details for your baby’s specific oral condition. If additional referrals are deemed necessary, such as to an infant chiropractor, infant CST, pediatric osteopathic physician or a pediatric physical therapist per examples you will be advised. There is often structural problems of skeletal or muscular such as torticollis or body asymmetry that are occasionally overlooked and require further evaluation. These are considered in your initial visit and information intake forms which will be completed before the exam. We include you in the evaluation, by taking pictures and answering your questions, so that you will be able to see if any tongue, lip, or buccal ties are present and understand the care process.
As you can now see the reasons for treatment or even no treatment can be singular or multiple.
A properly trained dentist or physician, who is aware of the functional anatomy of the infant’s mouth and important anatomical landmarks can perform treatment. If a frenectomy is indicated, the procedure happens during the same visit, so you won’t need to make an additional trip.
We use a Co2 laser which is ideal for this procedure as it causes minimal to no bleeding, or tissue charring and is minimally invasive. A specially formulated topical anesthetic will be placed on the tissue to be released, your baby will be swaddled, wear laser protective goggles and will be held gently by one of our team of caring providers. Parents have the option of staying in the room if they want to during the procedure. The actual procedure itself is very quick involving upto 5-10 minutes. Immediately after the procedure, mother can nurse her baby right after the procedure in one of our feeding rooms. You will leave with a set of post-operative instructions and wound care exercises.
My goal is to provide you with the ability to enjoy your breast or bottle feeding experience and to allow you and your baby to bond and enjoy this important time in your lives.
Wound Healing
A 2-week follow-up appointment to check on the healing and improvement of function. The revision site heals similarly to a canker sore, so your child may be fussy for a few days following the procedure. Some show immediate improvement with breastfeeding following the procedure. Other babies may need some time to learn how to use their newly released tongue. Exercises are recommended every 4 hours and will be one of the major factors in preventing reattachment, body work after therapy is recommended as well. Working with a lactation consultant can help get your changing breastfeeding relationship off to a good start.
Since the bottom of the tongue and floor of the mouth frequently touch, the site will occasionally reattach. To prevent reattachment, Dr. Mirkal recommends a specific aftercare regimen. Any reattachment requiring laser revision later is performed at no additional
charge.
So what does normal lip and tongue frenulum should look like?
When the upper lip is extended upwards and outwards there should be no blanching in the tissues or the surrounding areas, we are looking for a functional frenulum which will aid easy flanging of the upper lip while feeding. The infant should able to get his tongue under the mother’s breast easily and effectively able to draw out milk. We are looking for functional form. For tongue frenum , if the finger in passed under the tongue, it should be a smooth sweep and not a speed bump feel due to a restrictive frenum.
Fig 1,2,3 shows restriction in the ability of lip to flange. Fig4 Is a severely restricted anterior tongue tie extending to posterior tongue-heart shaped tongue.

Tongue tie symptoms in children
We prefer to wait till the age of 4 years to treat tongue / lip ties and any other oral restrictions past the age of 1 year. At 4 years and above we will numb the child with local anesthetic for the procedure and can offer nitrous oxide sedation. We recommend myofunctional therapy for children as an adjunct to frenectomy treatment. This applies to adult frenectomy as well.
Here are some most common symptoms to children
- Picky eating; food and texure aversions.
- Choking, vomiting, gagging on foods or liquids.
- Food falling out of mouth, using fingers to movie food in the mouth, pocketing food in the cheeks and food getting trapped in the palate, gums or cheeks.
- Speech issues; delay and or lisp.
- Digestive issues; constipation, “reflux” and IBS.
- Migranes and headaches.
- Behavioral issues and ADHD-like symptoms.
- Enlarged tonsils and adenoids.
- Sleep apnea, snoring or night terrors.
- Bedwetting or issues with toilet training.
- Dental and oral health issues; cavities and or bad breath.
- Chronic ear infections.
- Sinus or allergy issues.
- Scoliosis and torticollis.
- “Clumsiness” or affected posture.
- High palate.
- Malocclusions or crooked teeth requiring braces.
- Recessed chin.
- Jaw issues or TMJ, grinding of teeth.
Our story
Dr Mirkal’s son was born tongue tied in 2016 and she feels strongly about how a simple procedure can help moms to be able to breastfeed their infants and feels that it is critical for new moms to have a support system to help them in their new journey. We have several referral sources that help new moms with their challenges. Do not hesitate to reach out to us and let us know how we can assist you in your breastfeeding journey.